
On the cold evening of January 8, 1989, tragedy unfolded above the English countryside as British Midland Flight 92, a brand-new Boeing 737-400, suffered a catastrophic failure that would claim 47 lives and forever alter airline procedures and aircraft operations across the globe. The disaster, which came only weeks after the Lockerbie bombing, stunned a nation already reeling from aviation trauma. What happened in the skies above Kegworth, Leicestershire, was not simply a mechanical failure, but a tragic convergence of human error, miscommunication, and unfamiliarity with a new aircraft model.

A Routine Departure Turns into Crisis
Flight 92 was scheduled to travel from London Heathrow (LHR) to Belfast International Airport (BFS). The aircraft involved, tail number G-OBME, had only 521 hours of flying time and was the first of eight Boeing 737-400s delivered to British Midland Airways. It was equipped with CFM56 turbofan engines and configured with 156 all-economy seats. That day, it had already completed a return trip from Belfast uneventfully.
The cockpit was manned by an experienced crew with over 16,500 combined flight hours, though only 1,000 hours on the 737 model. On board were 118 passengers and eight crew members. Flight 92 took off at 19:52 local time and began a routine climb to 35,000 feet. As it ascended past 28,000 feet, disaster struck: a fan blade in the left engine detached, causing a loud pounding noise and severe vibration that resonated throughout the fuselage. Passengers near the rear saw sparks, smoke, and reported a burning smell—a clear indication that the left-hand (No. 1) engine was in trouble.
However, what followed was a catastrophic misjudgment. Inside the cockpit, the instrument readings were misinterpreted. The crew, believing the right-hand (No. 2) engine was the source of the issue, began throttling it back. The vibrations diminished—a deceptive result caused by reducing thrust from the fully functional engine rather than the damaged one.
The Fatal Decision to Divert to East Midlands
With uncertainty brewing, the pilots contacted the airline’s operations center, which advised them to divert to East Midlands Airport (EMA). Not only was EMA near the aircraft’s current trajectory, but it was also home to British Midland’s maintenance facilities. Flight 92 began its descent toward EMA and was cleared for approach to runway 27.
Throughout the descent, the Ground Proximity Warning System (GPWS) repeatedly warned of low altitude, indicating the aircraft had strayed below the glideslope. At just 900 feet altitude and 2.4 nautical miles from the runway, the left engine—a wounded workhorse still trying to deliver thrust—lost power completely. Now operating on no functional engines, the aircraft rapidly lost airspeed, falling below 125 knots, triggering the stick shaker that warned of an imminent stall.
Impact on the M1 Motorway and Destruction of the Aircraft
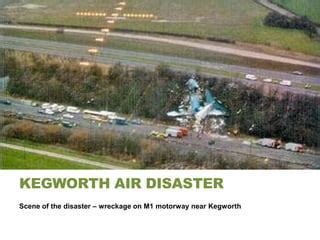
At 20:24, moving at a speed of only 115 knots, the aircraft’s tail and rear fuselage clipped trees on the embankment of the M1 motorway. The plane bounced and broke into three major sections after impacting rising ground. Remarkably, no vehicles on the motorway were hit, a stroke of fortune given the area’s typically dense traffic.
Thirty-nine people died instantly, with eight more succumbing to their injuries later. Among the 79 survivors, 74 suffered serious injuries. The pilots survived, although the first officer endured life-altering trauma. The event marked Britain’s last fatal crash of a UK-registered airliner.
The AAIB Investigation: A Catalogue of Human and System Failures
The Air Accidents Investigation Branch (AAIB) released its final report in August 1990, pinpointing the misidentification of the failed engine as the accident’s primary cause. It concluded that the flight crew had “reacted prematurely” and failed to fully analyze engine indicators before shutting down the right-hand engine.
The investigation revealed the crew had been influenced by outdated mental models. On older 737 models, the right-hand engine supplied air for cabin ventilation. Because smoke entered the cabin through vents shortly after the malfunction, and crew members reported this to the cockpit, the pilots assumed the smoke source was the right engine. Unbeknownst to them, the newer 737-400 split air supply between both engines, meaning the presence of smoke was no longer a reliable indicator.
Furthermore, critical visual confirmations from the cabin—passengers and crew witnessing flames from the left engine—were never passed to the cockpit. The captain, under the assumption that the issue lay with the right engine, even announced this over the intercom, which may have further discouraged contradictory reports from cabin crew.
The most devastating detail emerged during cockpit voice recorder analysis: when the captain asked, “Which engine is it?” the first officer began to say “It’s the le… it’s the right one.” The captain then instructed, “Throttle it back.” This verbal fumble may have sealed the aircraft’s fate.
Engineering Oversights and System Familiarity Issues
The incident also exposed shortcomings in training for new aircraft types. Despite having flown the Boeing 737 family, the crew had limited experience with the 737-400 variant, which featured redesigned systems such as engine bleed air and engine displays. The AAIB criticized both British Midland and Boeing for not emphasizing the crucial differences in their transition training.
Moreover, the engine itself—the CFM56—had undergone a fan blade redesign just before its adoption in the -400 series. The broken fan blade in the left engine, which initiated the disaster, was later linked to a manufacturing defect. As a result, mandatory inspections were subsequently introduced for all engines of the same type.
Regulatory and Operational Reforms Post-Crash
The legacy of Flight 92 was not in vain. Following the accident:
- Boeing revised the 737-400 flight manual to clarify changes in the air conditioning system and emergency engine procedures.
- Airlines adjusted simulator training to include unfamiliar aircraft variants and emphasized slow, deliberate engine failure assessments.
- Crew communication protocols were revised to ensure better collaboration between flight and cabin crew, with cabin reports given more structured priority.
- The brace position instructions were reworked to better protect passengers and were more clearly highlighted in safety briefings and seat cards.
- Overhead stowage bin standards were reviewed and improved to prevent them from detaching during impact, which had caused fatal head injuries in this crash.
One recommendation that remains unfulfilled was the call to introduce rear-facing seats for safety, a practice seen in military aviation and early commercial aircraft. Despite its potential to reduce injuries, public preference and airline economics have kept this measure from being implemented.

Conclusion: Lessons from Kegworth That Still Resonate
The Kegworth air disaster was more than a tragic crash; it was a sobering lesson in the complex interplay between human error, system design, and communication failure. The fact that a single incorrect assumption—left unchecked—led to the shutdown of a perfectly working engine, and the reliance on a damaged one, reflects the critical importance of structured decision-making under stress.
Today, commercial aviation remains the safest mode of transport, partly due to the hard lessons learned from such painful chapters in its history. The memory of the 47 lives lost in the fields beside the M1 motorway continues to influence flight training, cockpit instrumentation design, and emergency response systems across the aviation world.
Though Flight 92 never reached Belfast, its impact continues to ripple through the industry—an enduring reminder that progress often follows tragedy.








